The Pain System #1 - how our tissues respond to pain

This is the first of several blogs covering the pain system. In this blog we look at how tissues detect pain, whilst the next blogs will cover how the spinal cord and brain responds to these signals.
Pain is the reason most patients come to see us. There are other reasons: clicking, stiffness, swelling or pre-emptive injury prevention; mostly people who see us come because they are in pain.
The purpose of pain is to act as a warning signal. It occurs when the brain perceives damage or the threat of damage and wants to alert our body to take action.
Where does pain come from?
In most situations the perception of pain in the brain is fuelled by messages from the tissue where the threat is occurring, typically tendon, muscle and skin along with many other less well-known tissues such as fat pad and synovia.
All these pain-reporting tissues contain nerve receptors that alert the brain to what’s happening within the tissue due to stimuli such as stretching, pressure, heat, cold. As the stimulus increases so does the frequency of discharge of the receptors. Above a certain level of stimulus they start to report what we know as pain.
Slow onset injuries
With slow onset injuries the tissue is put under successive stress. As it starts to get close to the damage threshold it sends early warning signals. A result of these is that we experience pain but no actual tissue damage has yet occurred.
If we then to continue to load and stress the tissue we might go on to cause actual tissue damage and injury. So listening to early warning signals is a key part of managing the everyday load and stress on our body.
If we sit too long our back starts to ache due to prolonged compressive static loading on the tissue. So we get up and move around. If our achilles starts to niggle due to increased mileage we take a few rest days or drop our mileage down to let it settle before increasing at a more conservative rate. Well, in theory at least.
Sudden, acute injuries
With a sudden onset injury such as a sprained ankle or torn muscle a one-off load smashes through our pain and damage thresholds in one go. Pain and actual damage occur simultaneously
This type of pain tends to be far more intense and generally has a reasonable correlation with tissue damage. It is very effective in making us stop so we don’t cause further damage.
How does the pain threshold vary?
The load a tissue can tolerate before damage occurs gets higher the more load and stress we put through our body – this is why we train.
The achilles in a trained thirty-year old runner will normally have a much higher tolerance to loading than a seventy-year old sedentary person.
In ‘normal’ tissue the pain threshold shadows the damage threshold. As the tissue becomes stronger the nerve endings adapt and increase their threshold-level so it stays just below threshold for actual damage.
Conversely, when we damage tissue it becomes weaker. The load it can then tolerate before further damage occurs is decreased.
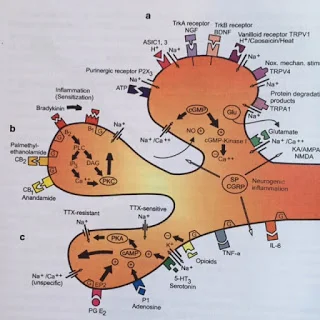
In this case the pain threshold is lowered. This occurs through a complex network of chemical and cellular interactions resulting in the production of a group of chemicals that directly lower the tolerance levels of the nerve endings. Below is a diagram of the various receptors of a nerve ending (Mense 2010).
For example when the skin is damaged by sunburn the pain tolerance of the nerve endings is lowered so that taking a hot shower causes significant pain. Taking the shower is not actually causing any further tissue damage, but the tissue’s threshold is now much lower.
When is pain helpful and when is it not?
This lowering of pain tolerance is useful in the early days of an injury so that we ensure tissue loading is well below tolerance load and healing is allowed to take place. As healing and tissue repair take place the tolerance threshold should rise back to ‘normal’ levels.
But this doesn't always happen.
Researchers have built up a good body of knowledge relating to the phases of tissue healing and repair and how long damage takes to repair under optimal loading conditions. We have a pretty good idea how quickly your injury should heal.
Sensitised Tissue
However the pain threshold can remain lowered even though full healing has occurred. The tissue is said to be sensitised. In this state pain messages continue at levels of load and stress that are not causing further damage and would have previously been fine.
This can also occur during healing if the pain tolerance doesn’t rise again in tune with the tissue getting stronger.
As the tissue remains sensitized and reports “false” pain the nerve endings adapt in another way. The number, density and sensitivity of nerve endings increase. There are more receptors to be stimulated by a given stressor and the pain messages sent to the brain are greater.
In sensitised tissue the lowered thresholds and increased number of receptors result in the tissue losing its capabilities as an early warning system and significant pain is produced even when loading is well below damage threshold.
Sensitised tissue e.g. the achilles, can be sore to touch, even though there is no actual tissue damage.
How do we treat sensitised tissue?
Applying sensible loading to sensitised tissue stimulates cellular responses which promote both structural change i.e. strengthening, along with lowering of both the number of nerve endings and their sensitivity.
The terms Mechanotherapy and Mechanotransduction are often used in this context.
Mechanotransduction refers to the process by which the body converts mechanical loading into cellular responses. These cellular responses, in turn, promote structural change. Mechanotherapy is then “the employment of mechanotransduction for the stimulation of tissue repair and remodelling.” Simples.
Case study – Recovering from a stress fracture in the fibula
A runner presented with a stress fracture in the fibula. After three weeks of initial rest from running the fracture site was pain free. We then closely managed a slow build-up of tissue load through running. Initially, after each increase in run length, the injured area was tender to touch and ached. We listened to the pain feedback to optimise the loading recovery programme. After eight weeks the runner was back to full training. Bang on target.
Case study – Poor initial management of a hamstring injury
A runner presented with an overloaded hamstring tendon – classic case of too much too soon. There had probably been structural damage but this was poorly diagnosed and treated. No guidance on loading levels was given. Subsequently the runner yo-yo’ed between resting, but not enough, then running for thirty minutes, which was too much.
I first saw the patient six months after the initial injury. At this time the hamstring was still weak and sensitised. We undertook a gradual loading program but this was difficult due to the sensitisation – the runner felt pain even though no tissue damage was being caused. Even when the hamstring was as strong as the other leg there was still pain with running short distances. We then worked to reduce the sensitisation through a running-based loading program.
Reference
Muscle Pain - Understanding the Mechanisms Siegfried Mense, Robert D Gerwin (Editors) Springer, 2010